
At 35 or 36, many couples are still told, “Relax, it will happen.” Sometimes it does. But when six months pass and every period feels like another disappointment, waiting a full year may not be the right advice.
If you are trying for a baby after 35, the first step is not panic. It is clarity. A fertility review can help you understand whether ovulation, egg reserve, semen health, timing, or another medical factor is delaying pregnancy.
At Dr Vinita Khemani’s clinic, the focus is not to push couples directly toward advanced treatment. The first step is usually a structured evaluation, careful counselling, and a plan that makes sense for both partners.
When should couples over 35 seek fertility help?
Couples where the female partner is 35 or older should usually seek fertility evaluation after six months of regular, unprotected intercourse without pregnancy. Earlier consultation is sensible if periods are irregular, there has been a miscarriage, or either partner has a known medical condition that may affect fertility.
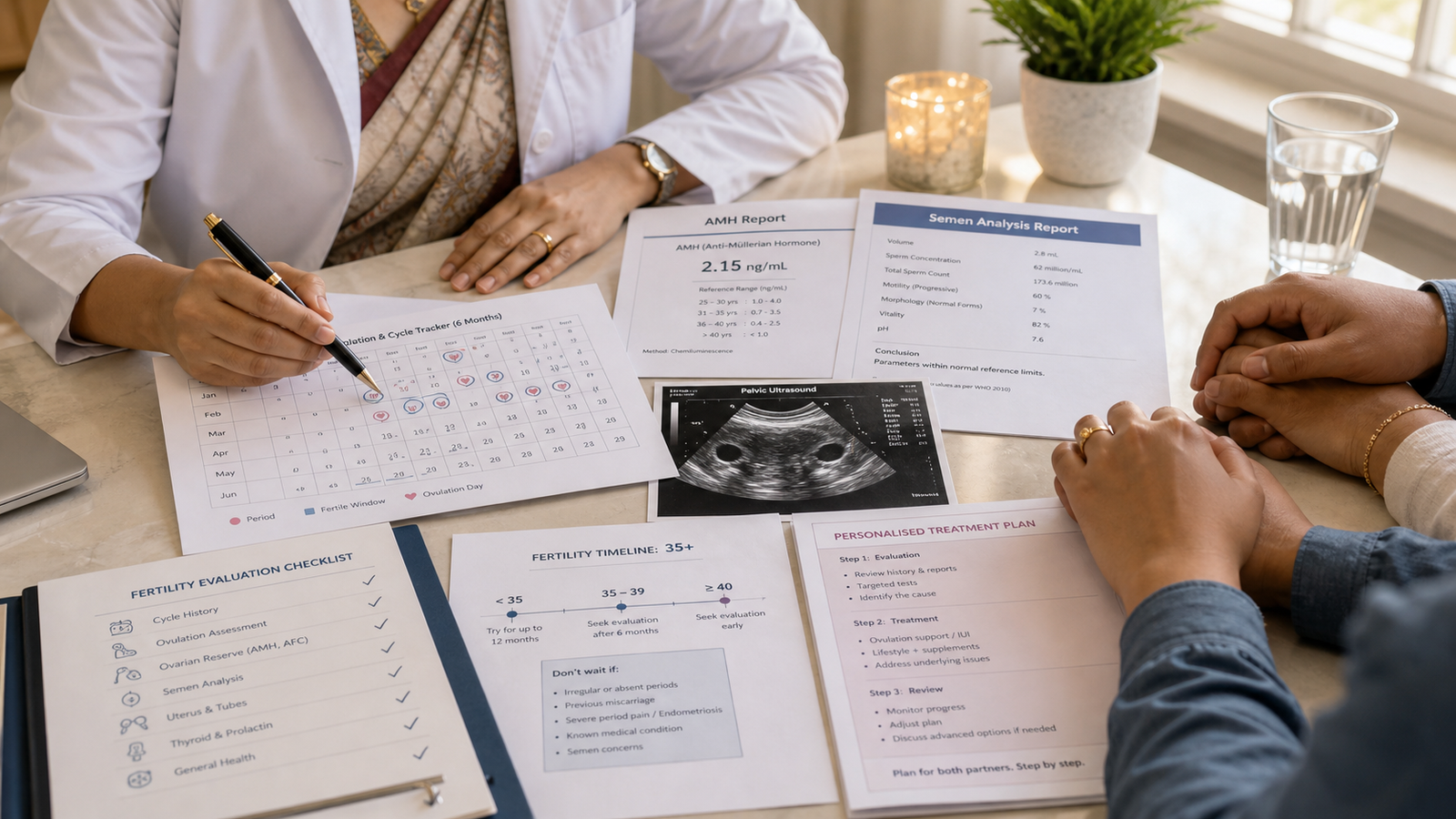
A simple way to understand the timeline:
- Below 35: evaluation is usually considered after 12 months of trying.
- 35 and above: evaluation is usually considered after 6 months.
- Over 40: evaluation should be discussed earlier, sometimes even before trying for long.
- Any age: do not wait if there are irregular periods, severe period pain, previous pelvic surgery, repeated miscarriage, or a known semen concern.
This six-month timeline is not meant to frighten couples. It exists because age changes the value of time. After 35, a few months of delay can matter if there is an ovulation issue, low ovarian reserve, blocked tubes, or male-factor infertility.
Why the “wait one year” advice can be risky after 35
The one-year rule is common, but it does not apply equally to every couple.
A 28-year-old with regular cycles and no medical history may be advised differently from a 36-year-old who has been trying for six months, tracking ovulation, and still not conceiving. The body may still be healthy after 35, but fertility assessment becomes more time-sensitive.
We often see couples who have already done many things at home. They have used ovulation apps, changed diet, taken supplements, followed cycle calendars, and timed intercourse carefully. Still, no one has checked whether ovulation is truly happening, whether the semen report is normal, or whether the ovarian reserve needs attention.
That is where the delay happens.
Trying every month without knowing the reason can become emotionally exhausting. It may also postpone a simple diagnosis that could have been identified earlier.
Fertility Management in Kolkata: what should a first evaluation actually include?
Fertility Management in Kolkata should not mean jumping directly to IVF or advanced treatment. A good first evaluation should answer one basic question: why has pregnancy not happened yet?
For couples trying after 35, the review should usually look at both partners, not only the woman.
1. Cycle pattern and ovulation clues
Your periods can reveal a lot. A 28-day cycle, a 35-day cycle, and a 50-day cycle do not tell the same story.
If periods are predictable, ovulation may be more regular. If periods are delayed, skipped, very light, unusually heavy, or unpredictable, ovulation may not be happening every month. In that situation, simply timing intercourse with an app may not be enough.
Important details include:
- How many days are there between periods?
- Has the cycle changed in the last 6–12 months?
- Is there acne, facial hair growth, sudden weight change, or hair fall?
- Is there severe period pain?
- Has thyroid, diabetes, or prolactin ever been checked?
- Are ovulation kits showing confusing or repeated positive results?
These small details help the doctor decide whether ovulation tracking, hormone tests, or ultrasound monitoring is needed.
2. Egg reserve and age-related planning
Ovarian reserve testing helps estimate how the ovaries may respond if treatment is needed. It does not guarantee pregnancy, and it should not be read like a final verdict.
Tests such as AMH, antral follicle count on ultrasound, and selected hormone tests may be advised depending on the patient’s cycle and history. The important point is interpretation. A report value without age, ultrasound findings, and clinical history can create unnecessary fear.
Some women come with a low AMH report and assume they cannot conceive. Some have a normal report but still need evaluation because pregnancy has not happened. Both situations need context, not panic.
3. Semen analysis for the male partner
This is one of the most commonly delayed steps.
Many couples first investigate the woman repeatedly while the male partner’s semen analysis is kept for later. That approach wastes time. Fertility depends on both partners, and semen parameters should usually be checked early.
A semen report looks at count, movement, shape, volume, and other factors. If there is a concern, it changes the plan. If the report is normal, it gives the couple one less thing to worry about.
Many people searching for “infertility doctors Kolkata” are not necessarily ready for treatment. They are often looking for someone who can evaluate both partners fairly and explain what is actually causing the delay.
4. Ultrasound and uterus-related assessment
A pelvic ultrasound may help assess the ovaries, follicles, uterus, and any obvious structural concern. Depending on history, the doctor may also discuss whether the fallopian tubes need to be checked.
Tube-related evaluation may be more relevant if there has been a previous pelvic infection, ectopic pregnancy, abdominal surgery, endometriosis symptoms, or a long duration of infertility.
The goal is not to do every test at once. The goal is to choose the right tests in the right order.
Seeing a fertility doctor does not mean you will need IVF
This fear keeps many couples away from medical help.
A fertility consultation is not the same as starting IVF. In many cases, the first visit is about finding out whether the basics are working properly: ovulation, egg reserve, semen health, uterus, tubes, and timing.
Some couples may need only better cycle tracking and timed intercourse guidance. Some may need medicines to support ovulation. Some may need further testing. Some may eventually need IUI or IVF, but that decision should come from proper diagnosis, not assumption.
This is why a structured review matters. It reduces guesswork and helps the couple make decisions calmly.
For evidence-based guidance, the American Society for Reproductive Medicine explains that fertility evaluation is generally recommended after six months for women aged 35 and above. ACOG also advises women over 35 to consider infertility evaluation after six months of trying, and women over 40 to discuss evaluation earlier. You can read these references from ASRM and ACOG.
When should you not wait even six months?
Some signs deserve earlier attention.
Irregular or absent periods
If periods come every 40–60 days, stop for months, or keep changing, ovulation may be irregular. Waiting for a full year in this situation may simply mean losing more cycles.
Previous miscarriage
One miscarriage can happen for many reasons. But repeated miscarriage, or difficulty conceiving again after a miscarriage, should be evaluated carefully.
Severe period pain
Pain that affects work, sleep, intercourse, or daily life should not be ignored. It may point toward conditions that can affect fertility and require proper assessment.
Known medical conditions
Thyroid disease, diabetes, PCOS, endometriosis, previous pelvic infection, pelvic surgery, or autoimmune conditions may change the fertility timeline.
Age over 40
After 40, it is better to speak with a doctor before spending several months trying without evaluation. The decision does not have to be aggressive, but it should be informed.
The emotional side of trying after 35 is real
Delayed pregnancy is not only a medical issue. It affects mood, marriage, confidence, family conversations, and daily life.
Some women start blaming themselves. Some couples stop attending family gatherings because they fear questions. Some avoid pregnancy announcements from friends because it hurts too much. These reactions are not weakness. They are common emotional responses to repeated uncertainty.
If fertility challenges are affecting your mental health, you may find this related article useful: The Psychological Impact of Fertility Challenges in Women.
This is also why early evaluation can be emotionally helpful. Even when the answer is not immediate, knowing the next step feels better than guessing silently month after month.
What to bring before your first fertility visit
A good consultation becomes easier when you bring the right information.
Carry or note down:
- age of both partners
- how long you have been trying
- dates of the last few periods
- usual cycle length
- previous pregnancy or miscarriage history
- ultrasound reports, if any
- AMH or hormone reports, if already done
- semen analysis, if already done
- thyroid, diabetes, or other medical history
- current medicines and supplements
- history of severe period pain, pelvic infection, or surgery
Do not worry if you do not have all reports. A doctor can guide which tests are actually needed. But avoid starting multiple fertility medicines or supplements on your own, because they may not address the real cause.
For couples with many basic doubts, this related guide may also help: 7 Common Fertility Questions Couples Who Can’t Conceive Ask.
What should a clear fertility plan answer?
A useful fertility plan should answer five questions:
- Is ovulation happening regularly?
- Is ovarian reserve appropriate for age?
- Are semen parameters healthy?
- Are the uterus and tubes likely to support conception?
- What is the most sensible next step for this couple?
That next step may be simple monitoring. It may be ovulation support. It may be further testing. It may be a discussion of treatment options. The right answer depends on the findings.
The World Health Organization describes infertility as a disease of the male or female reproductive system, which means both partners may need evaluation. You can read the WHO overview here: WHO Infertility Fact Sheet.
Internal service relevance
If you are over 35 and pregnancy has not happened after six months, another cycle of uncertainty may not give you the answer. A structured evaluation can help you understand whether the issue is timing, ovulation, egg reserve, semen health, or another factor.
You can visit Dr Vinita Khemani’s fertility service page to understand her approach to structured fertility management support in Kolkata.
FAQs
How long should I try naturally after 35 before seeing a fertility doctor?
Six months of regular, unprotected intercourse is usually enough time before seeking fertility evaluation after 35. The timeline should be shorter if periods are irregular, miscarriage has happened, or the woman is over 40. Bring cycle dates, previous reports, and partner details so the doctor can plan the right assessment.
Does seeing a fertility doctor mean I will need IVF?
Seeing a fertility doctor does not mean IVF will be required. The first step is usually to check ovulation, ovarian reserve, semen parameters, uterus, tubes, and timing. Treatment may involve simple monitoring, medicines, further tests, or advanced options only when clinically suitable.
What is the most successful treatment for infertility?
The most successful infertility treatment depends on the cause, age, ovarian reserve, semen parameters, tube status, and previous pregnancy history. IVF often has higher success potential in selected cases, but some couples may benefit from ovulation support, timed intercourse, IUI, or correction of an underlying medical issue first. A fertility evaluation helps decide which treatment is medically suitable instead of choosing the most advanced option too early.
Should my husband or partner do a semen analysis early?
Yes, semen analysis should usually be part of the early fertility workup. Male-factor issues can contribute to delayed pregnancy, and postponing this test may waste time. A basic report helps the doctor evaluate both partners fairly.
What fertility tests are usually advised for women after 35?
Fertility tests after 35 commonly include ovulation assessment, ovarian reserve testing, pelvic ultrasound, and selected hormone tests. The exact tests depend on cycle pattern, miscarriage history, medical conditions, and how long the couple has been trying. A doctor may also advise semen analysis for the male partner and further uterus or tube evaluation when needed.
What are the top 3 causes of female infertility?
The top causes of female infertility commonly include ovulation problems, fallopian tube-related issues, and age-related decline in egg quality or ovarian reserve. Endometriosis, uterine factors, thyroid imbalance, PCOS, and previous pelvic infection may also contribute depending on the patient’s history. After 35, a doctor may prioritise ovulation assessment, ovarian reserve testing, ultrasound, and partner semen analysis to avoid delay.
A practical next step
Trying for a baby after 35 does not mean you should assume the worst. It means you should not wait too long without knowing what is happening.
If pregnancy has not happened after six months, book a fertility consultation. If your periods are irregular, you have had a miscarriage, there is severe period pain, or you are over 40, seek help earlier.
A clear diagnosis can reduce fear, save time, and help you choose the next step with confidence.
Medical disclaimer: This article is for patient education only and does not replace a personal consultation. Fertility advice should be individualized based on age, cycle history, medical background, examination, and test results.
Have questions about this topic?
Book a consultation with Dr. Vinita Khemani to address your specific concerns and get a personalized care plan.